
When Taken with Meals: How Phosphate Binders Work
Introduction
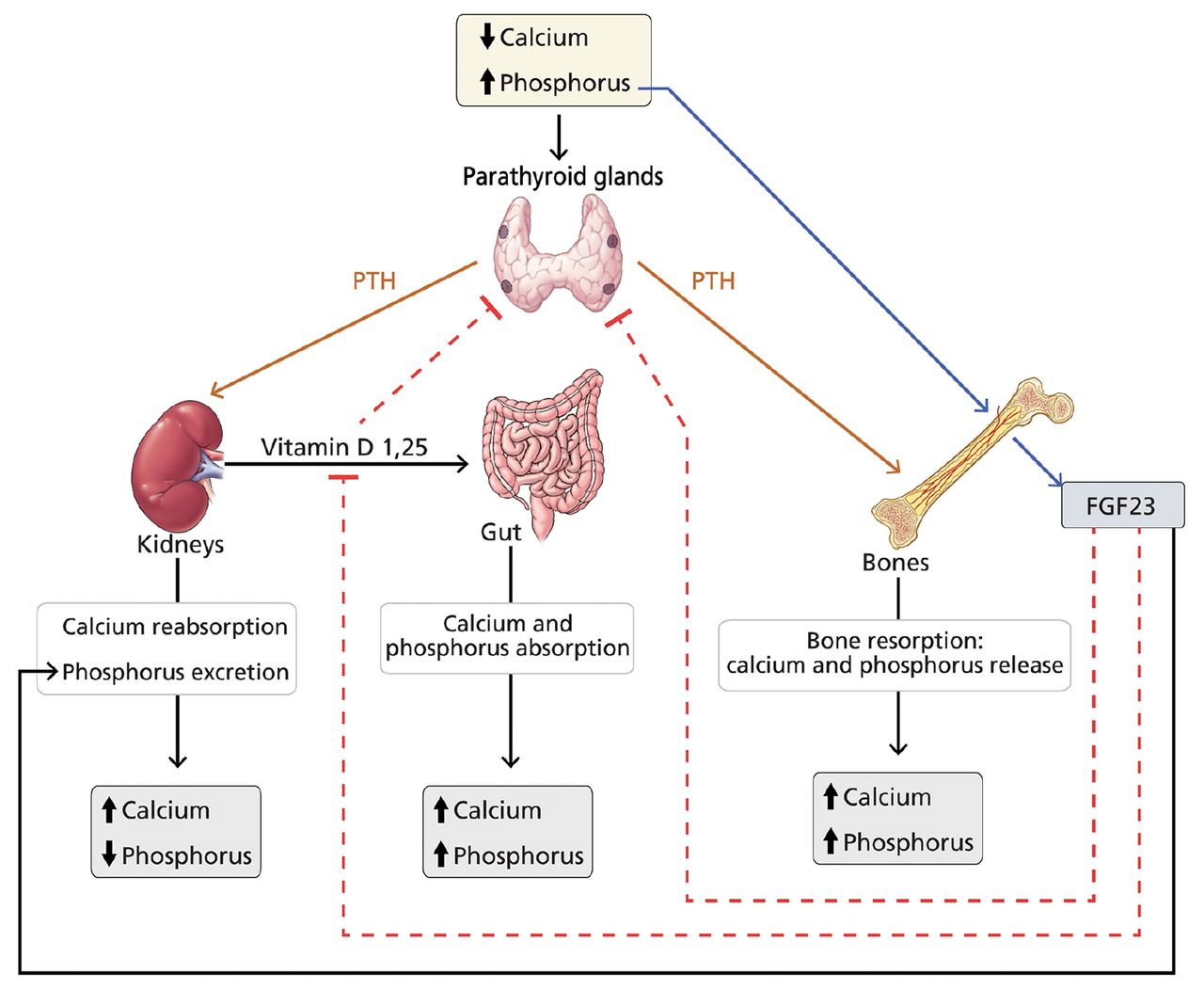
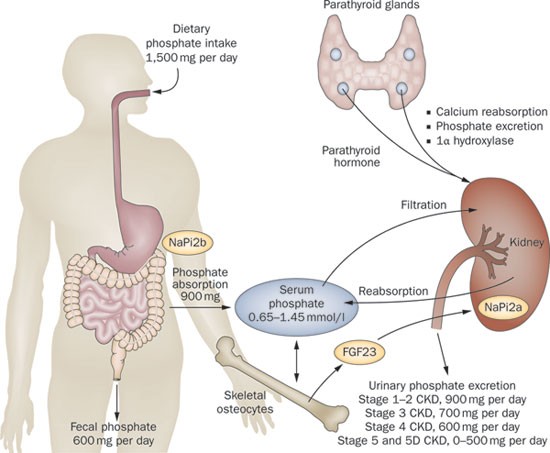
Phosphate binders are a class of medications commonly used in the management of hyperphosphatemia, a condition characterized by elevated levels of phosphate in the blood. This condition is particularly prevalent in patients with chronic kidney disease (CKD), as their kidneys are unable to effectively excrete excess phosphate. When taken with meals, phosphate binders play a crucial role in reducing phosphate absorption, thereby helping to maintain blood phosphate levels within a normal range. This article aims to explore the mechanisms of action of phosphate binders when taken with meals, providing a comprehensive understanding of their role in the treatment of hyperphosphatemia.
Mechanisms of Phosphate Binders
Phosphate binders work by binding to dietary phosphate in the gastrointestinal tract, preventing its absorption into the bloodstream. This process occurs primarily in the stomach and small intestine. The most commonly used phosphate binders include calcium-based compounds (e.g., calcium carbonate, calcium acetate, and calcium citrate), aluminum-based compounds (e.g., aluminum hydroxide), and sevelamer.
Calcium-Based Phosphate Binders
Calcium-based phosphate binders are the most widely used class of phosphate binders. They work by forming insoluble calcium-phosphate complexes, which are then excreted in the feces. When taken with meals, these binders bind to dietary phosphate in the stomach, reducing its availability for absorption in the small intestine. The effectiveness of calcium-based phosphate binders is influenced by several factors, including the dose, the timing of administration, and the presence of other medications or dietary factors.
Aluminum-Based Phosphate Binders

Aluminum-based phosphate binders, such as aluminum hydroxide, also bind to dietary phosphate in the gastrointestinal tract. However, their use is limited due to concerns about the potential for aluminum accumulation and its association with neurocognitive deficits. Aluminum-based phosphate binders are generally less effective than calcium-based binders and are recommended for patients who cannot tolerate calcium-based binders or have contraindications to their use.
Sevelamer
Sevelamer is a non-absorbable polymeric phosphate binder that works by binding to dietary phosphate in the gastrointestinal tract. It forms a complex that is excreted in the feces. Sevelamer is considered a first-line treatment for hyperphosphatemia in CKD patients, as it has a low risk of adverse effects and is effective in reducing blood phosphate levels. Unlike calcium-based binders, sevelamer does not interfere with the absorption of other nutrients, making it a suitable option for patients with malabsorption or dietary restrictions.
Timing of Phosphate Binder Administration
The timing of phosphate binder administration is crucial for optimal efficacy. It is generally recommended to take phosphate binders with meals or just before meals to maximize their binding capacity. This ensures that the binders are in contact with dietary phosphate for the longest possible time, thereby reducing its absorption. However, the specific timing may vary depending on the type of phosphate binder and the patient’s dietary habits.
Factors Influencing Phosphate Binder Efficacy
Several factors can influence the efficacy of phosphate binders when taken with meals. These include:
– Dose: The dose of the phosphate binder is an important factor in determining its effectiveness. Higher doses may be required to achieve adequate phosphate binding, especially in patients with severe hyperphosphatemia.
– Timing: As mentioned earlier, the timing of administration is crucial for optimal efficacy. Taking the binder with meals or just before meals ensures maximum contact with dietary phosphate.
– Dietary Factors: The type and amount of dietary phosphate can affect the efficacy of phosphate binders. Patients with high-phosphate diets may require higher doses or additional binders to achieve adequate control of blood phosphate levels.
– Other Medications: Some medications, such as proton pump inhibitors (PPIs) and certain antibiotics, can interfere with the absorption of phosphate binders, reducing their efficacy. It is important to consider these interactions when prescribing phosphate binders.
Conclusion
Phosphate binders are an essential component of the treatment strategy for hyperphosphatemia, particularly in patients with CKD. When taken with meals, these medications effectively reduce dietary phosphate absorption, helping to maintain blood phosphate levels within a normal range. Understanding the mechanisms of action, timing, and factors influencing the efficacy of phosphate binders is crucial for optimizing their use in clinical practice. Further research is needed to explore the long-term effects of phosphate binders and to identify the most effective and safe treatment strategies for hyperphosphatemia.
References
– Levey, A. S., Eckardt, K. U., Tsakiris, D., & Levin, A. (2012). Definition and classification of chronic kidney disease: a position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney International, 81(5), 651-660.
– Mandelbrot, D., Druey, M. M., & Block, G. A. (2006). Phosphate binders in the management of hyperphosphatemia in chronic kidney disease. American Journal of Kidney Diseases, 47(5), 733-744.
– Levey, A. S., Stevens, L. A., Schmid, C. H., Zhang, Y. L., Castro, A. F., Feldman, H. I., … & Coresh, J. (2009). A new equation to estimate glomerular filtration rate. Annals of Internal Medicine, 150(9), 604-612.
– Ferrario, C., & Druey, M. M. (2014). Phosphate binders in the management of hyperphosphatemia in chronic kidney disease. Seminars in Nephrology, 34(3), 223-233.



